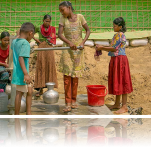
In the village of Divee in Gujarat, Dalit panihari (water women) report that when local government officials visit the village they are excluded from contact. Living for centuries as bonded laborers, the panihari — and their husbands, fathers, and sons, the chakars (field hands) — self-identify as slaves.